

Many women seek out a labiaplasty procedure to make them feel more comfortable wearing leggings, bathing suits, and other close-fitting clothing.
One of the most popular procedures that I do in my office is labiaplasty, a reduction in the size and reshaping of the labia minora or thin folds of skin that surround the clitoris and the vagina.
In fact, according to the American Society for Aesthetic Plastic Surgery, this procedure is incredibly popular, spiking over 200 percent in the past five years.
I’ve found that while many women are curious about labiaplasty and whether or not it would help them, many are embarrassed to talk about it. That’s why I put together these answers to your most common (& embarrassing) questions.
Different from the labia minora is the labia majora or outer “lips” of the vaginal area that grow hair (the labia minora sits within the labia majora).
Who has a labiaplasty?
Patients of all ages have labiaplasty, from teenagers to women in their 60s. Most of my patients come in and tell me they don’t like the appearance of their vaginal area. Most are not quite sure what can be done and want to understand their options.
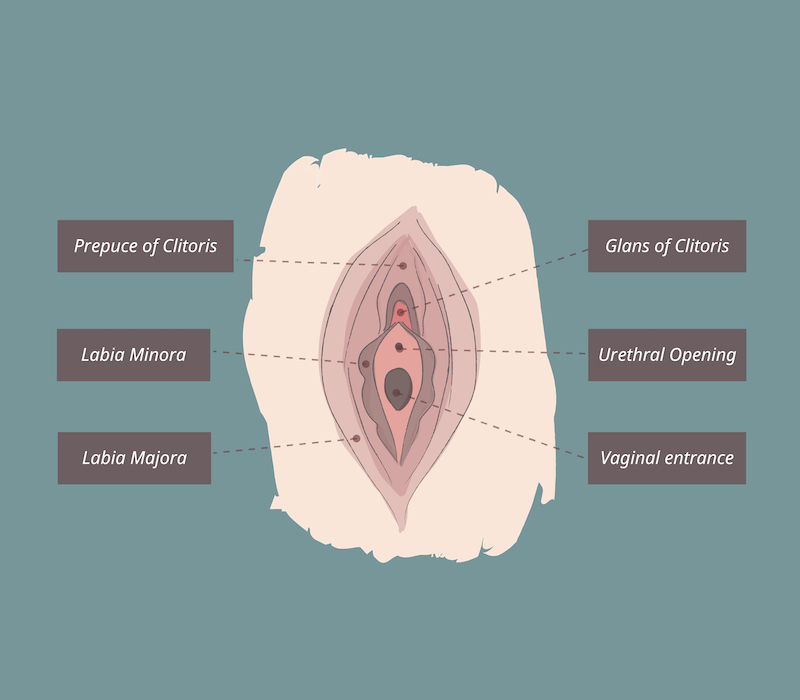
Labiaplasty can improve the appearance of the either the labia minora or the labia majora or both [see illustration above].
Typically, a woman will notice that she has bulging in the genital area that’s visible in yoga pants or other tight-fitting clothes such as bathing suits. Some women experience discomfort when exercising or interference with intercourse. This is due to excess tissue, where the labia majora has extra tissue and folds. It can be very localized or can extend above the clitoral hood. It can be present from puberty or noticed after childbirth. The labia majora can change as we age. Instead of being plump, the tissue can shrink, leaving the area deflated.
What exactly is done during the procedure?
During labiaplasty (which typically takes one to two hours), the excess tissue of the labia minora is trimmed and removed from the labia minora—while under local anesthesia and IV sedation. There are two ways to remove the excess tissue, either through an edge or wedge resection. Occasionally but rarely, the labia majora is also reduced.
“Edge” resections are very reliable and heal well. After healing there are no tell-tale signs of surgery. The excision is then closed using dissolvable stitches. Patients can usually go home after the surgery is completed.
There is also the option of a “Wedge” labiaplasty, where a V-shaped wedge is removed from both sides of the labia—with the remaining edges then stitched together. This method may have delayed healing. However, in certain patients it gives the best result. For most of my patients, I use the Edge resection approach for a pretty result.
If the labia majora is deflated plus/minus excess skin, there are several options:
- The labia majora can be inflated with fillers such as Juvederm or fat. This creates more cushioning of the labia majora.
- If there is extra skin of the labia majora, which needs to be removed, this labia majora excision should be done first, before the labia minora is corrected. Otherwise, the labia minora can develop a “splayed open” position.
How do you decide how much tissue to remove?
Labiaplasty is a very personal procedure and women have different aesthetic goals. There is no one right way for the labia to look. During your consultation, you’ll hold a mirror so you can see while I examine you. This way we can talk about the areas that bother you and you can explain to me how you would prefer your labia to look. This communication is very important and the “mirror exam” must be part of the consultation. Otherwise, I might not understand your goals.
I’ve been thinking about having labiaplasty, but I’m embarrassed to tell people I want to have it done. Does anyone have to know about it?
There is nothing to be embarrassed about. And no, you don’t need to tell anyone about it. The surgery is an outpatient one and the recovery is fairly straightforward with few side effects, if any. There’s no reason for anyone to know that you’re thinking about the procedure or having it done.
Like any aesthetic procedure, labiaplasty is an incredibly personal procedure. If you’re thinking about having it done—either because of how the area looks or because of irritation in the area—the decision to do it is yours alone.
My 17-year-old daughter has been talking to me about having labiaplasty. Is she too young to consider having this done?
Absolutely not. In fact, I perform this surgery on quite a few 17-year-olds. If a teenager has a prominent labia area that embarrasses her while changing in the locker room or in front of her friends or it shows through leggings (also sometimes referred to as a “camel toe”), surgery can be done with an extremely high satisfaction rate. There is no need for a teenager to go through life embarrassed about this particular part of her body.
I’m afraid of having general anesthesia. Is there any other way to have the procedure done without it?
Yes. In fact, I typically do the procedure as an outpatient procedure using local anesthesia with an IV sedative. I actually like my patients to be alert as, prior to surgery, I will make markings on their labia area while they’re lying down to indicate where I will trim. Then I have my patients look downward at these markings using a mirror they hold, and approve them, before starting the procedure.
How long will it be before I’m able to go back to work and sit at my desk?
After the surgery, it’s best to lie on the couch or bed as much as possible for first 48 hours. After surgery, my patients apply a numbing cream to the area several times a day as well as using ice packs on the area. The procedure isn’t painful and the numbing cream and ice keep you comfortable. Some patients take Tylenol or a low-dose narcotic. On a pain scale of 1 to 10, it feels like a 2 to most women. Urinating doesn’t cause pain. Patients can return to work on the third day after labiaplasty, assuming they don’t lift anything heavy at work.
Heavy lifting should be avoided for two weeks after surgery. Patients come to see me in the office each week for the first two weeks after surgery and then again in a month. (Of course, patients can reach me or my staff 24/7 with any problems or questions.) Sex can usually resume three to six weeks after the surgery.
Will I still be able to have children if I have this procedure?
Yes. As long as you’re not planning to get pregnant within the next year, labiaplasty will not interfere in any way with your ability to get pregnant and give birth to children vaginally. If you’re actively trying to get pregnant, it’s probably best to postpone the procedure as childbirth may affect the results.
For a consultation about labiaplasty, where I can address any additional questions you have about your personal goals, please call my office at 212-860-0670.